Symptoms
Symptoms of Fabry Disease
The symptoms associated with Fabry Disease are known to vary depending on age, sex and the location of the gene mutation. Amongst males, a distinction is now accepted to exist between ‘classic Fabry’ and ‘variant Fabry’ patients, due to the increasing number of people who present with some residual enzyme activity and as a result have delayed onset of symptoms or don’t present with all of the typical symptoms. The involvement of other environmental factors in the onset of symptoms and severity of symptoms is believed to be of importance but as yet has not been well established.
Females typically tend to have an level of enzyme inactivity, and as a result the onset of symptoms is later than for males, with symptoms becoming progressively worse with age. It has been recognised more recently that the response in affected females ranges from being totally asymptomatic to being as severely affected as males.
Symptoms become apparent during early childhood (age 4-10) and include chronic burning pain in the hands and feet, lack of sweating and gastrointestinal complaints. These problems can make physical activity difficult and are intensified during hot and cold weather.
Moving toward adulthood, proteinuria is and the implications this has on kidney function requires close monitoring. Cardiac involvement may also present during adolescence in the form of palpitations. Diarrhoea, nausea, vomiting, skin lesions and corneal changes are also common.
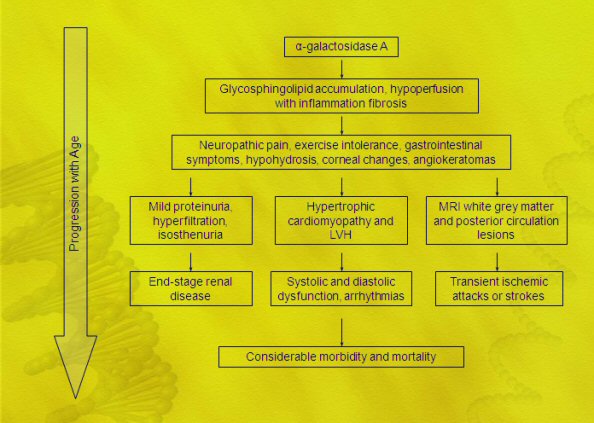
With increasing age, cardiac (hypertrophic cardiomyopathy, arrhythmias and impaired heart rate variability) and cerebrovascular abnormalities (stroke and transient ischemic attacks), together with a gradual deterioration of renal function, are very frequent.
For the purposes of assessing the severity of and the impact they have on quality of life, they have been divided here into primary (major clinical manifestations) and secondary (minor clinical manifestations). Primary symptoms are the effect of severe organ malfunction or failure that will eventually cause loss of life, whilst secondary symptoms are recognised as causing day to day discomfort, but are not generally life threatening.
Primary
- RENAL: Progressive reduction in kidney function is indicated by proteinuria and leads to renal failure. Birefringent lipid globules with characteristic “Maltese crosses” can be observed free in the urine and within desquamated urinary sediment cells by polarisation microscopy. Isothenuria, alterations of renal tubular functions, polyuria, gradual loss of cortico-medullary differentiation can be detected. Loss of kidney function is treatable using dialysis ultimately followed by kidney transplant, and kidney transplantation has proved quite successful if accepted as the new kidney will consist of cells producing a-galactosidase A. The mean age of death of 94 affected males who were not treated for loss of kidney function was 41 years (Desnick et al., 2000).
- CARDIAC: Cardiac involvement is signified by malfunctioning valves on the left side of the heart (mitral valve prolapse); thickening of the left ventricle wall (left ventricular hypertrophy); conduction causing arrhythmia and palpitations (supraventricular tachycardia, atrial fibrillation); angina and eventual cardiac failure. Abnormalities highlighted by ECG show a short P-R interval, ST segment changes and left-ventricular hypertrophy. Some of these abnormalities become apparent during adolescence and are not obviously linked with a progressive deposition and accumulation of protein. The development of heart deficiencies in Fabry patients and the exact mechanisms responsible for such requires further research.
- CEREBROVASCULAR: Patients can suffer from dizziness, vertigo, head pain, transient ischemic attacks, premature stroke. The frequency of stroke in classic Fabry males is significantly higher than that expected in the normal population, and similar trends are observed in females. Abnormalities can sometimes be detected by MRI.
Secondary
- ACROPARASTHESIA: Burning pain in fingers and toes. This can last anywhere from minutes to days. Pain can be more extreme during exercise, spells of hot and cold weather, fever and fatigue. Caused by peripheral nerve damage.
- ANHIDROSIS (HYPOHYDROSIS): Inability to sweat. This is due to GL3 accumulation in the sweat glands. This causes overheating during exercise, making physical activity during hot weather intolerable.
- ANGIOKERATOMA:Cutaneous vascular lesions presented as small reddish-purple skin marks which are one of the few visible signs of Fabry disease. The most apparent rash occurs on the lower back, but small marks occur sporadically across the body. These hardened or blocked blood vessels are the result of GL3 accumulation.
- CORNEAL WHORLING: This symptom does not affect vision, but can help diagnosis. A starburst pattern can be seen under slit lamp microscopy.
- GASTROINTESTINAL DISTRESS: Severe abdominal pains, possibly due to deposition of the glycosphingolipid in small intestinal vessels and in the autonomic ganglia of the bowel. Pain can resemble appendix/renal colic and diarrhoea is prevalent. A low protein diet, involving many small meals a day rather than few large meals may help to alleviate discomfort.
- PULMONARY DISTRESS: Bronchitis, wheezing respiration, dyspnea with alveolar capillary block. Smokers have been found to have greater airflow obstruction than expected from smoking alone.
- LYMPHOEDEMA: This involves localised fluid retention and tissue swelling, and may occur in the lower legs of some patients.
- MUSCULOSKELETAL DISTRESS: Avascular necrosis of the head of the femur, small infarct-like opacities in the femoral heads, involvement of metacarpals and metatarsals. Bony changes are characterised by multiple enthesopathic ossifications at the insertions of fibrous structures and articular erosions. This can be commonly misdiagnosed as arthritis or rheumatoid arthritis.
- FATIGUE.
- PSYCHOLOGICAL: The effects of all of the above listed symptoms when combined with treatment greatly affects the types of activity that Fabry patients can partake in. This can sometimes impair social interaction, and limit academic participation and professional opportunities. Greater interaction between patients can go some way to improving knowledge of the types of activities and occupations that are conducive to improved quality of life. Developments with regard to treatment and improved education for patients have the potential for safer and more independent administration of the drug within the homecare system. This can mean that treatment has less of an impact on patient’s lives.